


When Rebecca Emmanuel told me she slept two days inside water while fleeing from Boko Haram violence in her village in Gwoza of Borno state; got inflicted with a disease that might live with her forever; watched a neighbour burn her daughter’s wrapper because of the cough she now lives with, and neglected by a health system, then I understand what abandoned twice really means. First, she was abandoned in a life she never wished for in a remote IDP camp by the insurgency, then doubly abandoned by the government.
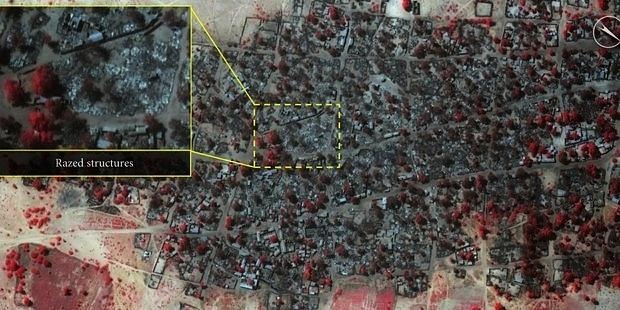
More than a decade after Boko-Haram insurgencies and violence began in Nigeria, Adamawa state has become home to about 3.7 million people, including 450,000 nomadic pastoralists still grappling with a shattered health system, which has put many nomads, including Adamawa’s internally displaced persons living with HIV and Tuberculosis, to being cut off from care. The IDP population are often known to be isolated and socially vulnerable to diseases such as TB and HIV infections. They are characterised by economic poverty, relatively little access to health services, increased morbidity and mortality, remote geographical location, social exclusion, and migration, among other factors.
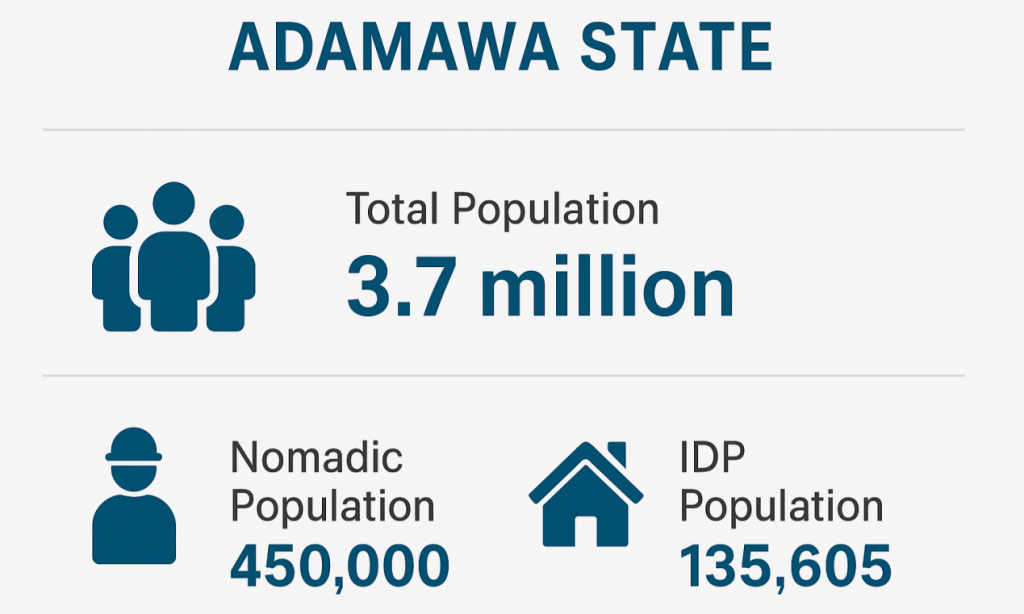
According to the IOM Displacement Tracking Matrix (DTM), as of October 2019, Adamawa has an estimated IDP population of 135,605, and as such, a considerable number of displaced people are impacted by the conflict. Many of these internally displaced persons (IDPs) in camps like Damare and Fombina, and many other IDP camps, have somehow been cut off from care. For Rebecca Emmanuel, an IDP Tuberculosis patient at the Damare camp, basic healthcare has become a distant dream.
“I got better, but it came back again”
A mother of three, Rebecca Emmanuel, is living in an internally displaced persons’ camp in Adamawa state. A decade ago, she was strong enough to farm and trade to support her family. Today, the 51-year-old struggles to stand without assistance or breathe without coughing.
Outside her hut made from canopies donated by the Norwegian Refugee Council, she lowers herself onto a white plastic chair beneath a tree, fighting for balance as another coughing fit sets in.
“Before, when I was still at home, I was very healthy. I was not feeling anything. It was in this camp that I started feeling weak and cold. I now wear a sweater. In my village, I didn’t need them.”
Ten years ago, Boko Haram attacks forced her family into the forest. She slept in rainwater, scavenged for food and lived in constant fear. It was under these conditions that she believes tuberculosis took hold of her body. Nine years ago, a local non-governmental organisation took Rebecca to a hospital in Numan, where doctors confirmed she had pulmonary tuberculosis. She was placed on medication, but treatment was neither regular nor sustained.

The worst-case scenario came when a neighbour treated her as untouchable. The decade of conflict has uprooted her from her home into this life in the camp, leaving her doubly “abandoned” – first by insurgency, then by a fractured health system.
Displaced families here live in almost complete isolation from basic health care. Clinics are scarce, and fear and stigma run rampant in the camps. As a result, TB and HIV diseases that are otherwise curable or manageable with treatment are now silently ravaging internally displaced persons (IDPs) who have already endured war and flight. Rebecca and other sick IDPs feel forgotten and systematically neglected.
“If not for Boko Haram, where would I have been caught with this illness?” she asks rhetorically.

What Data Says vs Reality Of the Health System
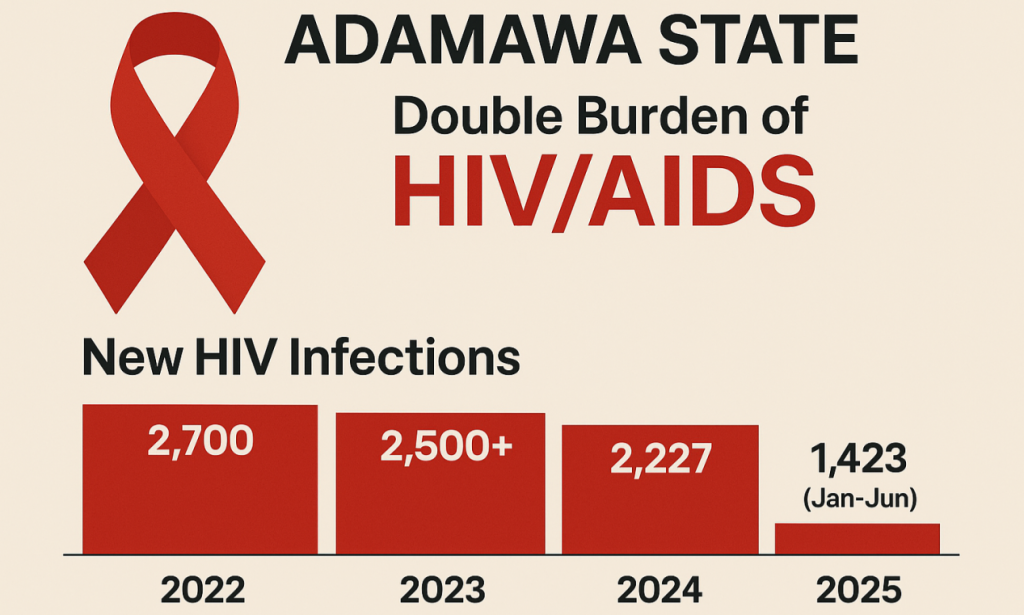
Official figures disclosed by Abdullahi Adamu, the Director of Research, Monitoring and Evaluation Agency (ADSACA), Adamawa state, have shown a persistent HIV epidemic. From 2022 to mid-2025, the state has reported roughly 8,850 new HIV infections, with over 2,700 in 2022, 2,500 in 2023, 2,227 in 2024, and 1,423 in the first half of 2025. About 40,000 people living with HIV are now on treatment, a number he said includes many in host communities as well as displaced people, though gender/age breakdowns are not provided. Remarkably, the viral suppression rate among those on therapy is high by 93%, reflecting effective treatment for those who can access it. However, the state still saw roughly 400 HIV-related deaths in 2024, and experts warn that overall prevalence is likely undercounted.
On tuberculosis, Adamawa state is recognised as one of the country’s highest-burden states despite its modest population. The state population of 3.7 million ranks among the top eight states nationwide for TB notifications, despite being only the 27th most populous.
Within the main TB screening area, which includes Malkohi, Mubi North and Gombi Local Government Areas, findings revealed that of 628 health facilities, only 109 offer DOTS – the standard TB treatment program, 32 have sputum smear microscopy, and a mere four have GeneXpert machines for rapid TB diagnosis. Every facility records TB tests in national registers, but by bringing such limited capacity to the camp front lines, many cases go undetected.
Dr Alobu Isaac, the Executive Director, Centre for Development and Reproductive Health, drew attention to this fact. He said many Nigerian health facilities remain ill-equipped to manage airborne diseases like TB, a situation he admits cost some health workers their lives. He lamented the “lack of proper infection-control mechanisms” and inadequate protection for staff.
“We don’t have data”
While disease spread quietly through the camps, official records remain empty. Findings revealed that there is no state-level data on HIV or tuberculosis cases among internally displaced persons in Damare, Fombina, Malkohi, Mubi North or Gombi IDP camps.
Neither the Adamawa State Ministry of Health and Human Services, the Adamawa State AIDS Control Agency (ADSACA), nor the National Agency for the Control of AIDS (NACA) can say how many displaced persons are living with HIV or currently battling tuberculosis. Investigation revealed that even where testing is carried out, no separate records exist for displaced people.
Repeated visits to the Adamawa State Ministry of Health in a bid to obtain records yielded little. During the first visit, the Director of Public Health, Mr Nuhu Yahaya, initially agreed to speak but declined when he realised the interview would be recorded.
On the second visit, the journalist gained access to the Ministry’s Permanent Secretary, Pharmacist Zirra Mathias, only after submitting documents seeking data validation and approval.
On the third visit, a Ministry staff member, Mrs Kenny Mykeal Dorcas, eventually responded, confirming that the data does not exist.
“Presently, our database as a state doesn’t have anywhere that we say these are specified records on IDPs living with HIV and Tuberculosis,” says Mrs Dorcas.
She further explained that all diagnostic testing relating to HIV and TB is logged under the nearest health facility. If a displaced person tests positive, the clinic might not record that they came from an IDP settlement. Dorcas bluntly put it: “If they didn’t specify that ‘I am from IDP camp, we don’t know. For now, the system has no separate tally of the displaced.”
This has not only made it nearly impossible to extract even an estimate of IDP HIV or TB case-loads within the state, but also exposed the Ministry’s poor on-ground surveillance for internally displaced persons.
The Ministry acknowledge the gap, but faults limited resources. Dorcas told the journalist, “Resource limitations are real, but we are expanding community outreach through partnerships. The major challenge is sustaining services in areas affected by insecurity. We acknowledge gaps in IDP-focused care, and we are working towards a stronger integrated response.”
“No one is helping us”

Six years into living with tuberculosis, Jamila Indallatu says the only help she ever sees in the camp is for fevers. TB, she says, has been ignored.
“I’ve seen campaigns for malaria and polio, but never for tuberculosis,” Jamila told Diaspora Africa. There is no help. Even if they are assisting, it’s just for the fever. For this illness (TB), they don’t assist people.
Jamila’s story is the same one told by her neighbour, Rebecca. She was diagnosed with TB six years ago and, unable to afford regular care, has been managing the disease herself. When she is too weak to work, she says fellow camp residents sometimes give her money so she can buy over-the-counter medicines to suppress the cough. She says she has never received free TB treatment or sustained medical support from humanitarian actors or the health system.
“If we could afford the medicine, we wouldn’t be living here in the IDP camp,” she said.
In an interview with Adamawa State NTBLCP Program Manager, Mr Andrew Misheli, he told the journalist the state currently has about 560-562 DOTs facilities within the state for TB patients, where health services are 100% free of charge. But also admit that the means of getting this free service to IDP communities are not provided at the moment.
“We have no money”
Forty kilometres away from the Damare camp is the Fombina IDP camp. The journalist met Elisabeth Bitrus.
Ten years ago, she escaped her village with her family during the Boko Haram insurgency. Tuberculosis struck her only after they settled in the camp. With no proper medical intervention, Elisabeth said she has been surviving the illness on her own terms. But surviving means she sometimes relies on self-made herbs or buys pills from the nearest local chemist, which is 20kilometers away.

“If you have the money, you can go to the facility to get the vaccine, but if you don’t, you just buy medicine at the chemist,” Elisabeth explains. The nearest TB referral centre is hours away by foot or motorcycle, impossible for someone like her since she can’t afford the cost of transportation.
The problems are identified, but what solution has been provided? What alternative mechanism has been put in place to help reduce the financial restraints on the internally displaced persons? Speaking to Diaspora Africa, Mr Andrew, the state NTBLCP Program Manager, disclosed that the state previously had what was called the local government TB and necrosis supervisors. He said the supervisors move around to take medications to some of the patients. But he further admitted that those services only extend to some communities within the state capital.
“For these particular IDPs that are outside this state capital, I may not be able to comment based on the fact that our service only covers communities within the state capital,” Andrew told Diaspora Africa
“At the moment, the program does not have any provision for any form of incentive, maybe transportation for them to be able to go to the facility to collect their medications. The only category of patients that enjoy such incentives are those with drug-resistant tuberculosis,” said Andrew
Consequently, TB patients in Damare and Fombina camp are already cut off from these free services, and completely left to survive on borrowed remedies, rely on self-made herbs, bought pills, and the occasional cash handout from neighbours.
All three women spoke of their pains and fear, as well as their anger and helplessness. The women feel abandoned by a system that claims to be inclusive, whereas its health system is one-sided. None of these women has been diagnosed with HIV (they have only TB), but it seems the same barriers block both epidemics. They speak of needing drugs, food, vaccines and information. They have no other options but to endure, hoping for charity.
“If you assist us, we will just say thank you. Bring us food aid and vaccines, and we will be thankful.” Elisabeth pleaded.
“Limited Facilities and Weak Access to Care”
Their stories only scratch the surface. Health workers and officials who visited the camps also confirm that TB and HIV are creeping problems, and that health services in these camps are very scanty.
“Nigeria’s TB fight remains fragile because of funding gaps, limited facilities, and weak access to care,” says Muhammad Pate, Nigeria’s Health Minister warned that funding gaps and limited healthcare facilities pose significant threats to Nigeria’s progress in Tuberculosis control.
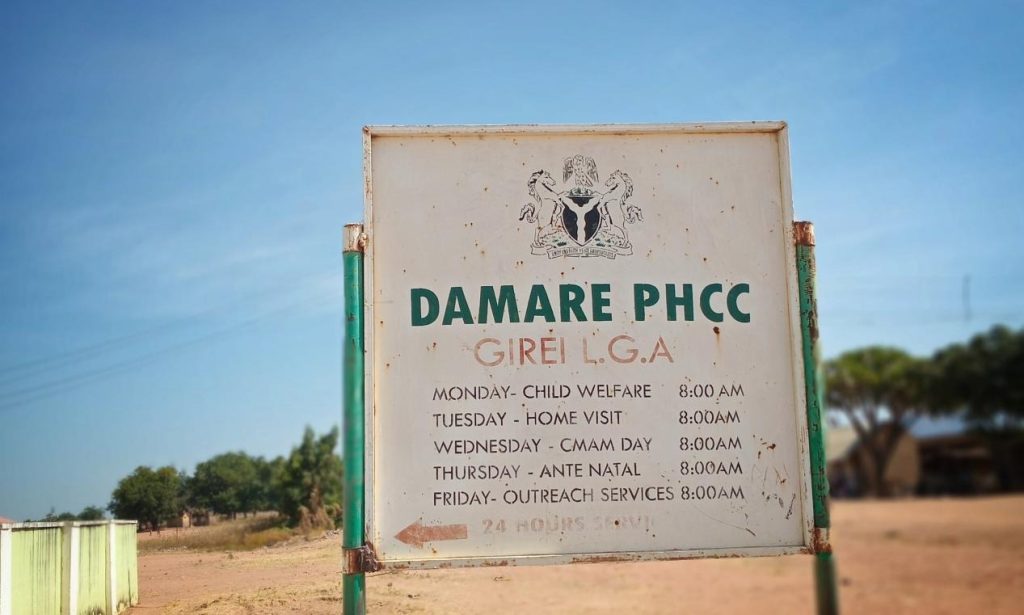
At Damare Primary Health Care Centre, the journalist met Nurse Aishat Musa, who manages primary care for the host community and the camp. Musa has worked at the facility for nearly five years and, like other health workers we spoke to, she described a service that is reactive rather than proactive.
“Generally, we are only offering the cases of HIV,” she says. “We do counselling. When we get a positive client, we call the NACA program officer, and they bring the drugs.”
Musa confirmed the facility has run just one outreach this year. An early-2025 testing event identified roughly five new HIV positive people across the community, but only one of them was from the camp itself. She added that the Adamawa State Ministry of Health occasionally asks her to mobilise residents for general screening.
“Sometimes we do sensitisation when the state is organising people, and we help.”
But these campaigns are sporadic and do not always include IDPs. On most days, she claimed the facility relies on individuals coming of their own accord…“Some come one by one, if they want to know their status,” she says. The positive ones are enrolled in care; the negatives go home. This pattern appears passive rather than active case-finding, which means many IDPs are likely to slip through the cracks.

“Let The Government Assist”
The situation surrounding TB seems more grave. Aishat Musa told the journalist that when they suspect TB, they collect sputum at the camp and send it to a laboratory in Yola inside the meter. But the follow-up is uncertain. To put it, even if TB is confirmed, there is no guaranteed supply of the six-month treatment at the camp.
“The drugs that were brought to them, because we don’t have drugs here, so when this drug finishes, where are we going to get the drugs to continue for them? Let the government assist with the drugs since we can meet them.” Musa says simply.
Budget on paper versus reality
Investigation revealed that in the 2025 Appropriation Bill presented by Governor Ahmadu Umaru Fintri, the state budgeted 486.2 billion naira. In the breakdown shared publicly, the Health Ministry line was allocated 22.3 billion under the 2025 budget. Out of the 22.3 billion allocated to Health line, 50 million naira was said to be approved for TB service across the state, but till now, the state NTBLCP Programme Manager confessed that only 2 million naira has been released so far.
“If you go through the budget item by item, on the approved budget for the state minister of health, under the TB program, you will notice that about 50 million was approved for TB services to procure medications and consumables for TB services. And to this date, no ‘kobo’ has been released to the activity. From the available records, right from April when I came in till now, only two million naira has been released, and the only funding the program has received from, out of the budget from the state government, is probably when they are organising maybe the World TB day,” says Andrew Mishelia, state TB programme manager.

The state TB program faults the government’s over-reliance on donor funding for carrying out active TB services across the state. With just 2 million naira, he said it is not enough to cover any activities because nothing is going to happen. But the consequences are grave; shortage of TB medications, consumables, reagents for several weeks, out-of-stock syndrome and laboratories running out of cartridges for Gene Expert.
“Part of the budget was supposed to go into the procurement of the drugs. But nobody is working towards that. Everybody is waiting for what is coming out of the donor fund,” says the state TB programme manager.
“If funding is provided by the state government, we can make additional procurement for the states to curtail this out-of-stock syndrome. But the funding is not even coming from the state government at all. So you can’t even make any extra provision for your state. You have to rely on what comes in from the national, and if what comes in from the national is inadequate, then everybody suffers.” Andrew Mishelia told Diaspora Africa
In most cases, the state TB program relies on little from the National government or donations from neighbouring states.
There is a need for sensitisation
Against this backdrop, camp residents remain alarmingly vulnerable. A survey of nomadic communities in Adamawa found that the correct understanding of TB/HIV was very low. Only 13.6% of respondents knew that HIV and TB complement each other. The rest believed the diseases were unrelated or even the same.
More troubling, during an interview with Kenny Mykeal Dorcas at Adamawa’s Ministry of Health, she admitted to the state’s poor surveillance on IDPs, and that many camp residents simply never present at the clinic at all.
“You are supposed to have picked from your own findings that when I went around, they said they (IDP) don’t even go to the facility because they don’t know they have TB. They need to be sensitised,” said Mrs Dorcas.
In other words, if people do not seek care, they remain invisible. Practically, Adamawa’s health bureaucracy has yet to figure out how to capture the scale of the problem among displaced people, which paints a picture of total neglect.
“She burnt my wrapper”
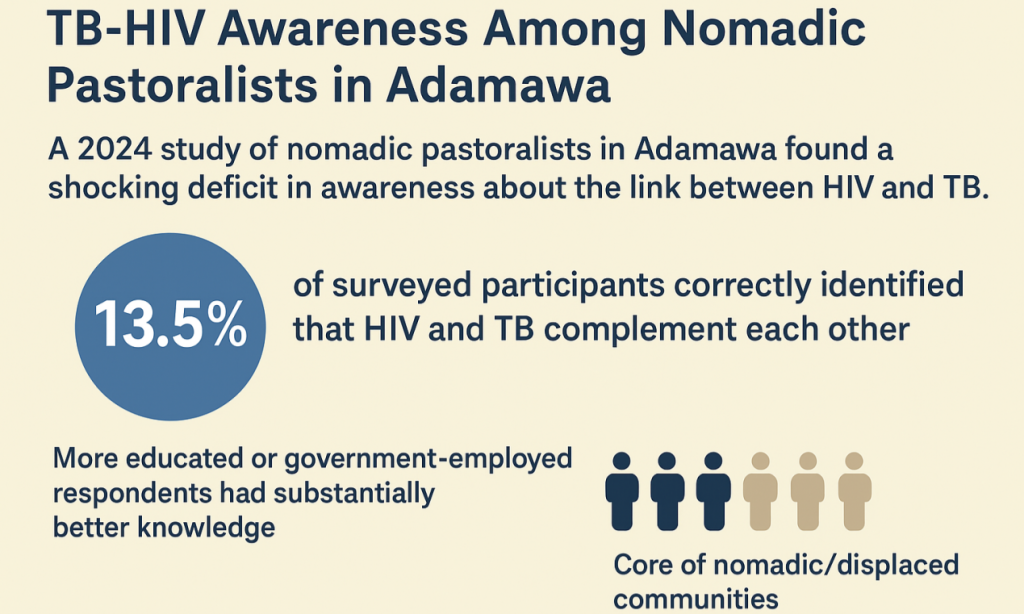
Physical barriers are compounded by stigma and misinformation due to a lack of proper awareness among the internally displaced persons. A 2024 study of nomadic pastoralists in Adamawa found a shocking deficit in awareness about the link between HIV and TB. Only 13.5% of surveyed participants correctly identified that HIV and TB complement each other. The study further showed that respondents who were better educated or government-employed had substantially better knowledge. Meanwhile, the core of nomadic/displaced communities was among those least likely to know about TB-HIV co-morbidity. As a result, experts warn that a lack of awareness breeds stigma and misinformation.
Rebecca Emmanuel still remembers the sting of a small kindness turned sour. A month earlier, before this report, a neighbour in the camp gave birth. Rebecca gathered one of her daughter’s wrappers, still in use at home and offered it as a gesture of support. It was a simple act, the kind mothers in crises extend to one another.
But days later, she walked past the woman’s room and saw something that unsettled her. The new mother had packed up the wrapper, tossed it outside, and instructed her children to burn it. Shocked, Rebecca asked for the cloth to be returned since her daughters could still use it. Instead, the woman insisted that the children wash it, but that was just a gesture to settle the storm. Moments later, they set it on fire.
“That’s how they see us, as disgusting,” says Rebecca.
When she confronted the woman, she was dismissed. “You already gave it to me,” the neighbour replied, shutting down any further conversation.
Rebecca walked away, disturbed and powerless. In the camp, she says, there is no one to report such indignities to. All she can do is endure, cling to patience, and hope that one day God grants her a better life.
Deep-rooted stigma and misinformation would or might further prevent them from care-seeking or asking for help. Many of the camp dwellers still believe Tuberculosis to be a curse or a death sentence. Within Adamawa’s nomadic communities, only about 15% of men and 10% of women correctly understand the link between HIV and TB, and over half believe TB cannot be cured.

Hunger and Poverty Competing With Treatment
“Tuberculosis thrives where poverty, displacement, and overcrowding intersect, and that is exactly the reality in many IDP settlements in Adamawa,” said Dr Idris Abdullahi, an Infectious Disease specialist and expert
Fractured health services and stigma are just two out of the many challenges the IDPs are facing. Poverty is another visible barrier here in the camps. At every corner of the camps, there is evidence of food insecurity, lack of proper shelter, tents packed shoulder-to-shoulder, damaged toilets, and the mental trauma caused as a result of displacement are part of the burdens that eclipse their distant health concerns.

When we asked what help they needed the most, our interviewees’ first answers were food and money, not drugs. Their priorities reflect their survival instincts. Only a well-nourished person might be able to better resist the infection. Conversely, studies have found that chronic malnutrition and crowded living conditions create an ideal breeding ground for Tuberculosis. Whatever health-seeking journey they might likely embark on, it will compete with these more immediate needs than the treatment.
Efforts In The Past
Notably, in recent years, Nigeria’s Institute of Human Virology (IHVN), supported by the Global Fund, has bolstered TB detection across the country. Between 2021 and 2024, IHVN-funded programs screened over 3.5 million people and diagnosed over 350,000 TB cases. But IHVN’s outreach has mostly hit cities and large towns while it lags in reaching the poor and rural communities.
At the moment, the State TB programme is partnering closely with some CBOs that are working specifically on IDPs. According to Andrew Mishelia, state NTBLCP program manager, the CBOs go to these camps and see these patients, screen them based on the case definition of tuberculosis, screen samples taken via the nearest health facility, and then link them to a laboratory facility that offers TB testing. These partners’ initiatives include Superbill Community Initiative, the Leprosy TB Relief Initiative, the Global Fund, and the Jenna Health Foundation. But the state NTBLCP says those services are limited to certain local governments.
In a phone call conversation with Humpiya Bassoon, Technical Officer for Jenna Health Foundation, he spoke on the foundation’s partnership with Adamawa state TB programme. He said the organisation was established in 2012, and since then, it has been working on several projects with the state and so on. It’s an organisation that has been working on TB by targeting key and vulnerable populations. However, he also confirmed that the organisation’s services are strictly confined within certain local government areas based on available funds.
“The IDP project is run in five local governments: Yola North, Yola South, Mubi North, Mubi South, and Fufore. These are the areas where the project covers,” said Humpiya Bassoon
Gaps and Way Forward
Global targets loom. Nigeria endorsed the UNAIDS 95–95–95 strategy, aiming by 2030 to diagnose 95% of all HIV cases, treat 95%, and achieve viral suppression in 95% of those on treatment. However, Adamawa is far from reaching that goal. Despite free ART programs, an official admitted that new infections keep rising. Experts blame donor cuts after the 2023 U.S. halt of new PEPFAR funding for Nigeria.
But achieving the 95-95-95 target by 2030 depends on reaching the last 10 per cent of people. Those living in remote communities, conflict zones, and displacement camps. If states like Adamawa struggle, Nigeria as a whole risks missing national and global milestones.
Nigeria’s NTBLCP proudly announced a 93% treatment success in 2023, but these figures track only those who reach treatment centres. If IDPs aren’t counted at all, their outcomes are left out of national tallies.
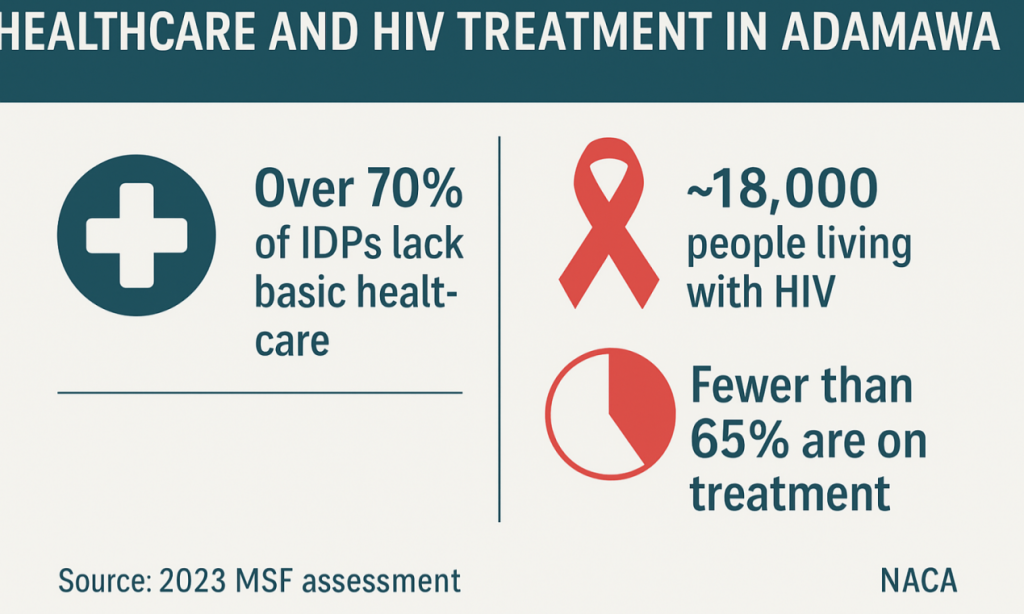
A 2023 MSF assessment found over 70% of IDPs lack basic healthcare; NACA figures show ~18,000 people living with HIV in Adamawa, with fewer than 65% on treatment, concentrated among hard-to-reach and insecure communities.
The Executive Secretary, Adamawa State Agency for the Control of Aids, Dr Boniface Gundiri, said “the agency is strategising with new skills to combat the spread of the virus. I’m happy to announce that, yes, research is on, and I think by year 2030, the 95-95-95 target will be achievable. With these issues of commitment of the government, more especially the Adamawa state government, in terms of HIV and TB response.” But his comment does not reflect the reality in the state.
Andrew Mishelia spoke about the lack of state funding and over-dependence on donor funds, but he also suggested a possible solution to address the crisis. He emphasised strengthening partnerships and collaboration with organisations, while he disclosed that the state only has two partnerships at the moment.
“Right now, we work through IHVN as a sub-recipient of their funds. Some of our partners are also sub-recipients of the Global Fund. At the moment, there is no other partner outside of this arrangement that is willing to or able to support or fund our activities,” says Andrew, state NTBLCP programme Officer
One other way the state government can maximise the funding gap, according to Andrew Mishelia, is through collaboration with other programs; the HIV program and malaria program, by leveraging on their platforms to extend health services to other locations with the minimum resources available.
“If the HIV program has some funding for maybe two or three supervisionals to carry out, and then malaria has funding for maybe two or three in a month, why not move together as a unit? That means we can relatively do six local governments in a month, rather than one or two. It will go a long way if other partners can leverage our platform to extend their services to those communities.”
Andrew also suggested the need to do more advocacy to the government. He thought that there were implications for reliance on donor funding, and why the state government should create a structure of its own.
“Each state government needs to work towards ownership of the program in the state, increase the funding for the program in the state, so that it will supplement whatever is coming from donor funding, not to over-rely on donor funding because of the recent experiences we have had.”
A generation of Adamawa’s displaced is growing up vulnerable. There are many factors at play here: clinics under-stocked, tests too few, people too poor and uneducated, stigma and response too sporadic. Without routine immunisation or check-ups, TB cases and undiagnosed HIV will continue to run unchecked.
Grace Nyako, a community Health Volunteer in Fufore LGA, told the journalist…“What these people in the camps want is simple. They want a nurse who comes when she says she will, medicines that are available all month, and someone who listens without judgment. When these basic things fail, people turn to traditional remedies or give up treatment entirely.”
This is a wake-up call to Nigeria’s state governments to prioritise their health sectors by providing enough funds and creating an independent structure instead of over-reliance on donor funding.
Writer: Bankole Taiwo James
Editors: Amaka Obioji, Chimee Adioha
Cover Image: Diaspora Africa
“This content received support from the Thomson Reuters Foundation as part of its global programme aiming to strengthen free, fair and informed societies. Any financial assistance or support provided to the journalist has no editorial influence. The content of this article belongs solely to the author and is not endorsed by or associated with the Thomson Reuters Foundation, Thomson Reuters, Reuters, nor any other affiliates”.
