

Every year, Nigeria’s federal government allocates billions of naira to train doctors, nurses, pharmacists, and other health professionals across its public universities. The students pay a fraction of the true cost. The state, through subsidised tuition, publicly funded teaching hospitals, and clinical placement infrastructure, carries the rest. Then, systematically and at scale, the graduates leave. They take up positions in the United Kingdom, the United States, Canada, Australia, and the Gulf. They save lives there. And Nigeria, the country that paid for their formation, is left holding the bill.
This is not a new story, but it has never been told in the right way. The conversation around Nigeria’s medical brain drain has been dominated by familiar framings: it is a tragedy, it is a symptom of governance failure, it is the rational choice of individuals escaping dysfunction.
All of this is true. But there is a harder, more specific question underneath those narratives, one that cuts through grievance and into fiscal accountability. What is the actual monetary value of the human capital Nigeria is exporting? And who, precisely, is benefiting?
When you run the numbers, the answer is as clarifying as it is uncomfortable. Nigeria is, in effect, running one of the world’s largest publicly subsidised talent pipelines, not for its own citizens, but for the healthcare systems of wealthy countries that neither fund the training nor compensate the source.
The Scale of the Exodus
The data has become impossible to ignore in recent years. According to a November 2025 report by Nigeria’s Federal Ministry of Health and Social Welfare, a total of 43,221 doctors, nurses, pharmacists and medical laboratory scientists emigrated from Nigeria between 2023 and 2024 alone. That is not a trend. That is a haemorrhage. Within that period, migration of health workers across all cadres surged by 200 percent.
In 2024 specifically, 4,193 doctors and dentists left. For context, Nigeria graduates roughly 4,399 doctors in a full year. The country is, in effect, replacing barely one year’s cohort of graduates while simultaneously losing almost an entire cohort to emigration, and that is before accounting for the gap between those trained and those retained in previous years.
The nursing picture is even starker. A 2025 peer-reviewed study in SAGE Journals, authored by Gabriel Samuel and Jonah Japhet Haruna, found that approximately 42,000 nurses left Nigeria between 2022 and 2024. The National Association of Nigeria Nurses and Midwives has separately confirmed that 75,000 nurses have left Nigeria since 2017.
These are not workers who simply changed jobs. They are credentialed professionals, trained at public expense in Nigerian universities and teaching hospitals, who are now delivering care in British wards, Canadian clinics, and American emergency rooms.
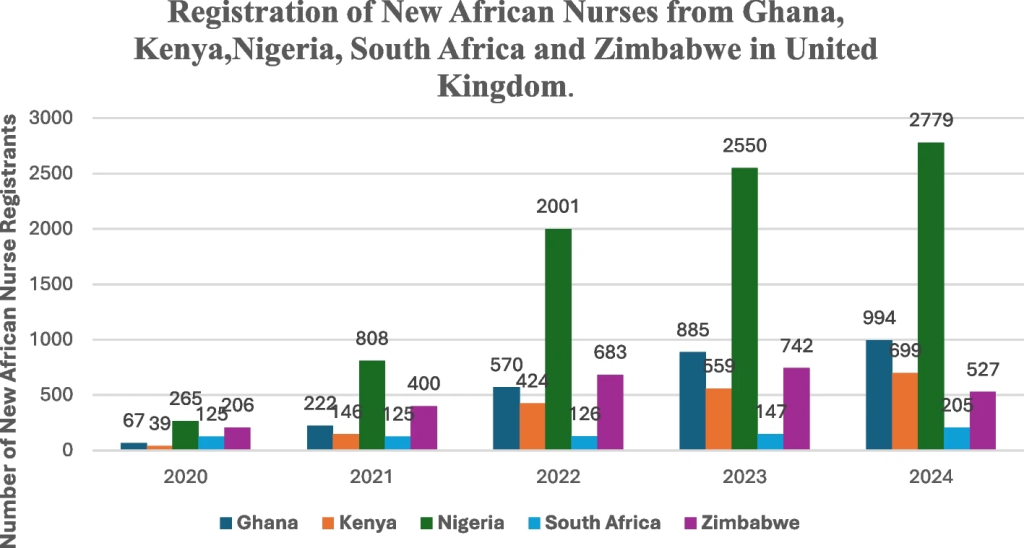
The United Kingdom is the primary destination. According to data from the Nursing and Midwifery Council of the UK (NMC), Nigerian nurse registrations in Britain increased by 343.9 percent between 2021 and 2024, from 808 new registrations to 2,779 in a single year. Nigeria now accounts for the largest portion of the NHS nursing workforce from sub-Saharan Africa. A 2024 BusinessDay report confirmed that Nigerian-trained nurses joining the UK workforce hit an eight-year high, with Nigeria listed among the top three countries with the second-largest increase in skilled health and care visas to Britain.
The Cost Nobody Calculates
Here is where the story gets specific — and uncomfortable. Training a medical doctor in Nigeria is heavily subsidised by the state. A student at Ahmadu Bello University, one of Nigeria’s largest federal medical schools, pays roughly ₦70,000 to ₦100,000 per session in tuition — a figure so low it is almost symbolic.
University of Calabar charges as little as ₦39,000 per session. These fees bear no relationship to the actual cost of delivering a six-year medical education: the laboratories, the teaching hospitals, the consultant faculty, the clinical equipment, the administrative infrastructure. A 2021 study published in the Pan African Medical Journal estimated that the total cost of training a doctor in Nigeria — including tuition, living support and associated costs — ranges between $21,000 and $51,000. The difference between what the student pays and what the training actually costs is borne almost entirely by the Nigerian state and, ultimately, by Nigerian taxpayers.
Now compare that with what the United Kingdom would need to spend to produce the same doctor domestically. The UK’s Personal Social Services Research Unit (PSSRU) at the University of Kent — whose estimates are cited by the British Parliament — puts the cost of training an individual doctor from the start of medical school through to the end of foundation training at approximately £327,000.
The UK government’s own figure, cited in a 2017 consultation on medical training, placed the total cost of training a doctor in England at £230,000, with roughly £163,000 representing non-repayable public grants — money the government never gets back, regardless of where the doctor subsequently works. Training a nurse in the UK, per the PSSRU estimates referenced in Parliamentary written answers, costs approximately £67,000. The arbitrage, when you lay these figures side by side, is staggering.
When the UK recruits a Nigerian-trained doctor, it acquires a fully qualified health professional, trained to international standards over six years, for free. No tuition grant. No clinical placement subsidy. No bursary. No foundation year salary. The British state collects a ready-made worker that would have cost it between £163,000 and £327,000 to produce itself, and pays nothing for the training.
Apply that logic to scale. Between 2023 and 2024, over 43,000 Nigerian health professionals emigrated. Even if we take a conservative assumption, applying only the nurse training cost of £67,000 to the nursing majority of those emigrants, the implied value of training that the UK and other destination countries received, at zero cost, runs into the billions of pounds. If we apply the doctor training cost of £163,000 to non-repayable public grants for even a fraction of the physician emigrants, the transfer of publicly funded human capital from Nigeria to Britain alone dwarfs Nigeria’s total annual health budget.
In 2024, Nigeria’s federal health allocation was approximately ₦1.336 trillion, about 4.6 percent of the total budget. This fell far short of the 15 percent minimum that African governments committed to under the 2001 Abuja Declaration. At a state level, a BudgIT report found that Nigerian states spent an average of just ₦3,483 per person on health in 2024, with no state reaching ₦10,000 per capita.
A country spending less than ₦10,000 per citizen annually on healthcare is simultaneously exporting, at no charge, thousands of fully trained professionals whose domestic production would cost a wealthy country hundreds of thousands of pounds each.
What It Is Doing to Nigeria
The consequences are not abstract. They are, at this point, measurable and severe. Nigeria needs a doctor-to-population ratio of at least 1:600, according to WHO recommendations. Its current ratio is 1:5,000, according to the Minister of State for Health and Social Welfare. The nurse-to-population ratio stands at 1:2,000 against a WHO recommendation of 1:300. A Nigeria Health Watch analysis found that Nigeria would need approximately 400,000 doctors to meet international standards — it has around 66,000. Experts have estimated it would take Nigeria at least 20 years to close the gap at current production rates, even if emigration stopped entirely — which it shows no sign of doing.
A 2025 study published in Cureus found that nearly half of all Nigerian medical graduates had emigrated within 15 years of qualifying. The same study documented a cascade of system-level consequences: understaffed hospitals, eroded mentorship capacity, impaired specialty training pipelines, and widening inequities in rural access. When senior doctors leave, they take with them not just their clinical labour but years of institutional knowledge that cannot simply be replaced by hiring more graduates.
The Lancet put it plainly in a 2024 commentary: “Nigeria has a density of only 1.83 skilled health workers per 1,000 people, which falls far short of WHO’s recommendation of 4.45 per 1,000 people. With a population expected to reach 263 million by 2030 and a growing trend of medical professionals leaving the country, this problem is poised to worsen unless addressed effectively.”
The people who are left behind are not abstractions. They are the patients in overcrowded government hospitals, cared for by exhausted doctors who work far beyond safe clinical limits. They are the women in rural areas where the nearest nurse has moved to Leeds. They are the children whose post-natal care is delivered by health workers so stretched that errors become inevitable.
Towards a Different Conversation
None of this is an argument for restricting the movement of individuals. The doctors and nurses who leave Nigeria are not doing anything wrong. They are making rational decisions in the face of poverty wages, dangerous working conditions, crumbling infrastructure, and a government that has consistently allocated less than five percent of its budget to health.
Nigerian Polling Organisation found that 88 percent of medical doctors in Nigeria were already seeking opportunities abroad, a figure that has only grown since. These are people, not units of human capital, and their choices deserve to be respected. The argument, rather, is about where the accountability lies, and with whom.
Nigeria’s government must be held accountable for its chronic underfunding of the health system. The Abuja Declaration, signed by Nigerian leaders in 2001, committed member states to allocating at least 15 percent of their annual budget to health. More than two decades later, Nigeria has never reached that target.
The highest allocation under the current administration was 5.75 percent in 2023. The 2026 proposed allocation is 4.2 percent. A country that will not fund its own health system cannot credibly claim to be a victim of brain drain alone — it is also failing to create the conditions that would make staying a reasonable choice.
But destination countries also bear a responsibility that the current discourse consistently lets them escape. The bilateral agreements that govern migration and labour should be redesigned to include explicit training compensation mechanisms — arrangements under which countries that systematically recruit health workers from Nigeria pay into a fund that supports Nigerian medical education, hospital infrastructure, or the salaries of those who remain.
This is not a radical idea. It has been proposed in academic and policy circles for years. What is radical is the continued preténce that importing publicly funded talent from a health-impoverished country carries no obligation whatsoever.
Nigeria is also not without leverage, if it chose to use it. It trains health workers who are globally competitive, globally sought, and globally in short supply. That is a resource. The question is whether Nigeria’s government has the political will to treat it as one — to build bilateral agreements that tie cooperation in other areas to concrete commitments on health workforce compensation, to use the WHO framework as a platform for demanding accountability rather than as an aspirational document, and to invest meaningfully enough in the sector that staying begins to look like a real option.
The Bill Is Already Due
There is a version of this story that ends with a call for more research, a working group, a task force. That is not this version.
The data is already in. Nigeria trained them. Britain hired them. The bill, in lives not saved, in hospital wards not staffed, in children not vaccinated, in women who gave birth without a skilled attendant, is being paid for every day by Nigerians who never chose to be part of this exchange. Forty-three thousand health workers in two years.
A doctor-to-patient ratio that is 1,000 percent below WHO recommendations. A health budget that has never reached half the commitment made in Abuja over two decades ago.
The question is not whether this constitutes an injustice. The numbers make that clear. The question is who will finally say it plainly, and force the people responsible — in Abuja and in London — to reckon with what the ledger actually shows.
Writer: Victor Ejechi
Editors: Beatrice Nwoko, Chimee Adịọha
Illustration: Diaspora Africa